




Karli Swenson, University of Colorado Anschutz
The obstetrics staff was surprised the first time it happened in June 2025. A pregnant woman who was dependent on methamphetamine arrived at the hospital in labor. She showed an image of graffiti spray-painted on a bridge in downtown Denver that read “Have your baby at Lutheran.” She was scared, and in pain, but wanted to be somewhere she felt safe asking for help.
Not long after, it happened again.
Another laboring woman with the same image on her phone. Apparently, word was getting around that this labor and delivery unit did things differently.
The women showed up at the hospital months after providers there had participated in a training program about caring for pregnant patients with substance use disorders.
After delivery, both women engaged with recovery services, which include meeting with peer support, attending recovery meetings and sometimes moving into either detoxification centers or sober housing. They remained connected to these support systems, which are designed to improve outcomes for parents and families affected by substance use disorders.
Substance use disorders are common in general, but also common among people who get pregnant. Many pregnant people report experiences of judgment, stigma and discrimination in healthcare settings. Research has found that fear of negative treatment can discourage patients from disclosing substance use, engaging in prenatal care or seeking treatment services.
These barriers may contribute to a disturbing trend: Overdose has become a leading contributor to maternal mortality. In Colorado, accidental overdose is the second-leading cause of death among people during pregnancy and the first year after birth. Between 2016 and 2020, 33 people in Colorado died of overdose during pregnancy or in their first year after birth.
I have spent much of my career studying substance use during pregnancy. For three years, I worked with the Colorado Perinatal Care Quality Collaborative, a public health organization dedicated to improving outcomes for parents and babies in Colorado, to develop and implement programs aimed at improving perinatal substance use care.
Stigmatized care for people who use substances
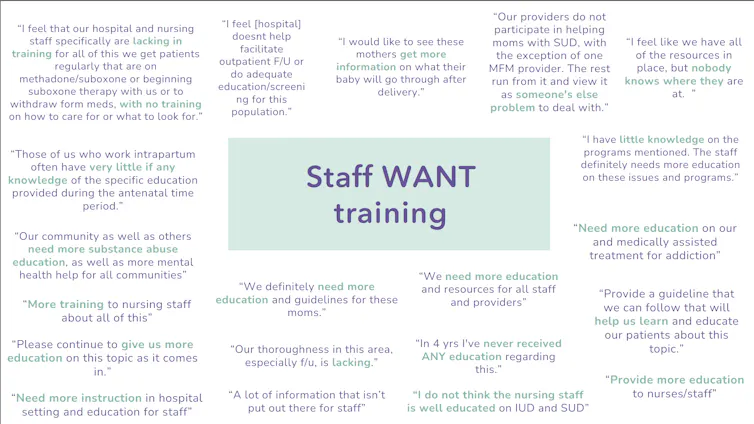
I worked with a team at the collaborative to survey labor and delivery nurses about their co-workers’ attitudes toward pregnant patients with substance use disorders.
Many nurses reported hearing their colleagues using stigmatizing language and dismissive behaviors. Some providers described assumptions that patients with substance use disorders were irresponsible, dishonest or less deserving of empathy than other patients. Others reported witnessing judgmental comments, gossiping, staff intentionally violating patient privacy, staff wanting to punish the patients for their actions and denial of pain management during labor.
These findings aligned with a growing body of literature documenting stigma toward pregnant people with substance use disorders across healthcare settings.
In my own experience with these providers, I’ve learned such attitudes are rarely held with malicious intent. Many clinicians work in demanding environments, care deeply about infant well-being and may have limited formal training in addiction care. In short, they believed that shaming the moms may help their babies.
One survey participant said, “We definitely need more education and guidelines for these moms.”
Training to change minds and practice
The survey results led us to develop a training for obstetric and neonatal healthcare professionals. We partnered with HardBeauty, a Colorado organization led by women with lived experience of substance use and recovery.
Between 2023 and 2025, 1,454 healthcare professionals completed the training we developed in 33 hospitals, birth centers and community organizations in Colorado. Participants included nurses, physicians, midwives, social workers, lactation consultants and nursing educators. Many of the hospitals required their staff to complete the training as a way to address known gaps in care.
The training was 90 minutes either in person or on Zoom. For 45 minutes, the training focused on the trauma that predisposes people to substance use in pregnancy and the increasing prevalance of substance use in pregnancy during the opioid epidemic in Colorado.
Though few studies include the perspectives of patients with substance use directly, one study found that 87.1% of the participants with substance use in pregnancy experienced emotional abuse, 74.2% experienced physical abuse and 51.6% experienced sexual abuse. Knowing how patients start using substances to numb the pain of experiences like these helped participants empathize with patients who use substances.
We discussed real clinical scenarios, practiced talking to patients in ways that wouldn’t stigmatize them and learned strategies for connecting patients with local treatment and recovery resources.
Most importantly, the healthcare providers who participated spent the second half of the training in small groups with moms in recovery from HardBeauty who serve as peer support specialists. These moms told open, honest and raw stories of abuse, trauma, substance use, recovery, relapse and motherhood. They also shared their own experiences of being too afraid to ask for care while pregnant out of fear of losing their child. These conversations were difficult. Many ended in tears and hugs between healthcare staff and the peer support specialists.
The healthcare providers in our trainings later told us that these interactions made them see the patients who find themselves pregnant while suffering from a substance use disorder as human.
One participant said the training helped them to “see a story behind a patient and understand their perspective.”
Another wrote, “They are humans and deserve love and understanding just like anyone else.”
The survey results showed significant improvements in knowledge about substance use in pregnancy, maternal mortality and barriers to care.
Another healthcare provider said “going into this training I was frustrated that I was required to go to another training; by the end I was thankful.”
Our results showed that participants reported greater empathy toward pregnant and postpartum people with substance use disorders than they had before the training. They learned that addiction is a treatable medical condition rather than a moral failing. They also described increased confidence discussing substance use with patients, identifying treatment resources, arranging referrals and responding to stigmatizing comments from colleagues.
One person’s survey response reflected the goal of the training: It “changed how I will approach patients in the future.”
Building trust and compassionate care
The two pregnant women who came to Lutheran after seeing that spray-painted message on the bridge were looking for caregivers they could trust.
Healthcare systems frequently measure outcomes such as length of stay, complications, readmissions and treatment utilization. Those metrics matter. But the experiences that patients have while receiving care matter, too.
When people feel respected, heard and supported, they are more likely to return for care, engage with treatment and recommend services to others. The long-term effects of these interactions between clinicians and new moms can be difficult to quantify, but they may influence entire communities.
If new moms with a history of substance use think the healthcare system is a safe space, they are more likely to attend recovery services, go to their postpartum appointments and take their child to their pediatric visits.
Read more of our stories about Colorado.
Karli Swenson, Postdoctoral Fellow, Department of Pediatrics, University of Colorado Anschutz
This article is republished from The Conversation under a Creative Commons license. Read the original article.
















{kind=link}